About Physiobreathe training
Over the past decade, respiratory muscle training (RMT) has grown steadily in popularity, thanks to a growing evidence base, and the support of a number of systematic reviews and meta-analyses. However, most healthcare professionals still have only a rudimentary knowledge of the theory and practice of RMT, and require support in order to implement the treatment effectively. This is the gap Physiobreathe training is intended to bridge. The techniques will therefore be of interest to the following:
- Primary and secondary care physicians
- Physiotherapists
- Nurses
- Rehabilitation professionals
- Exercise scientists
- Academic clinical teachers
- Expert patients
Introduction
Recent systematic reviews and meta-analyses show that specific respiratory muscle training (IMT) improve exercise tolerance, dyspnoea and quality of life in a wide range of clinical conditions, including:
Furthermore, the improvements are similar in magnitude to those that can be attained following whole body exercise training (see O'Brien et al, 2008 and Smart et al, 2012. This makes IMT an extremely powerful and cost-effective tool for the management of patients with cardiorespiratory illness.
As well as COPD and CHF, there is growing evidence that IMT produces clinically useful benefits for patients with:
- Respiratory disease
- Asthma
- Bronchiectasis
- Cystic fibrosis
- Restrictive chest wall disorders
- Neurological and neuromuscular disease
- Obesity
- Ageing
- Diabetes
- Renal failure
- Iatrogenic myopathy (pharmacological and mechanical ventilation)
- Obstructive sleep apnoea
- Vocal cord dysfunction and inspiratory stridor
- Weaning failure following mechanical ventilation
- Post-surgical respiratory impairment
The Physiobreathe training system employs a two-stage process to optimise the benefits of IMT:
Stage 1: Foundation training employs evidence-based techniques that optimise the training stimulus to maximise initial training benefits. (link to Foundation training section below). Foundation training lays the foundations of strength, power and endurance. These foundations provide functional improvements in their own right, but the outcome can be improved still further by placing a functional layer onto these foundations.
Stage 2: Functional training builds upon the benefits of Foundation training by applying functional training methods to IMT. Functional exercises challenge the inspiratory during postural control, core stabilisation and trunk rotation roles. For more information on Physiobreathe's functional training approach go the "The Book" (link) and "Videos".
For many patients, Foundation training is all that's required, but for others, additional benefits are possible by undertaking IMT in conjunction with functional movements. These movements mimic everyday challenges such as lifting, carrying and overhead arm movements.
Foundation training

How do we train the inspiratory muscles? By applying the tried and trusted principles of resistance training using a device that is akin to a "dumbbell for the diaphragm" (see figure). Research has shown that inspiratory muscles adapt in the same way as other muscles.
Foundation training is undertaken using an inspiratory muscle trainer such as the POWERbreathe Medic - this is the "dumbbell". As is the case with any form of weight training, there's a right and a wrong way to lift the weight if you want to enjoy maximal reward for minimal effort. The following sections guide you through the scientifically validated principles for successful Foundation training.
Note that during the Foundation phase of training, there are no special body movements or positions; instead, the inspiratory muscles are isolated to maximise their response to training. During the Functional phase of training training, the inspiratory muscles are integrated into functional movements.
 The following information is taken from the book 'Respiratory muscle training: theory and practice'. If you want to know more, then you can buy this comprehensive guide to breathing training by following this link.
The following information is taken from the book 'Respiratory muscle training: theory and practice'. If you want to know more, then you can buy this comprehensive guide to breathing training by following this link.
For information on contra-indications, follow this link.
Breathing technique:
Relearning normal efficient breathing strategies is the "essential groundwork" that underpins Foundation IMT. Accordingly, expert readers are encouraged to ensure that patients receive appropriate diaphragm breathing training as part of their Foundation IMT. Further guidance can also be found in 'Respiratory muscle training: theory and practice'. A useful Physiobreathe breathing pacer App is also available – this sets the duration of each phase of breathing, the breathing frequency, counts the number of breaths, and the duration of the practice session.
Breath volume: Although muscle is a very adaptable tissue, training adaptations are also highly specific to the nature of the training stimulus. Adaptations elicited by IMT are specific to a number of characteristics of the training stimulus, including the lung volume at which training takes place. The practical implication of this is that IMT should be undertaken across the widest range of lung volume possible, i.e., from as close to residual volume as possible, to the point at which it is impossible to inhale any more. Failure to do this will lead to sub-optimal adaptation at some lung volumes, which is particularly important in patients who hyperinflate when minute ventilation increases. An important consideration in maximising tidal volume (VT) during IMT is the training load; loading too "heavily" can compromise VT that can be achieved, and the amount of work that can be undertaken during training, which will also impair the training response. This impairment occurs because VT has a strong influence upon the amount for work done per breath, and the most important determinant of the ability to inhale deeply is the training load (McConnell & Griffiths, 2010). Functional weakening of the inspiratory muscles during inhalation means that if the load is too high, the inspiratory muscles are not be able to overcome the load at higher lung volumes (where the inspiratory muscles are weaker), despite maximal effort. The heavier the load, the more severely the breath is "clipped".
This means that the training load must be set with these factors in mind. The figure below illustrates the interrelationships of inspiratory muscle strength, lung volume, and training load, as well as the effect of fatigue on the VT that can be achieved. Note that the breath volume is clipped progressively earlier in the breath with increasing loads.
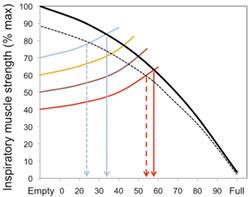 Figure 6.2. The interactions between inspiratory muscle strength (black line), various training loads (40, 50, 60, and 70% of inspiratory muscle strength [coloured lines]), and the breath volume that can be achieved during training, as well as the effect of fatigue (dotted lines). For example, at 40% , it is possible to inhale to around 60% of vital capacity, whereas at 70% it is only possible to inhale to around 35% of vital capacity. Adapted from Breathe Strong, Perform Better, Human Kinetics.
Figure 6.2. The interactions between inspiratory muscle strength (black line), various training loads (40, 50, 60, and 70% of inspiratory muscle strength [coloured lines]), and the breath volume that can be achieved during training, as well as the effect of fatigue (dotted lines). For example, at 40% , it is possible to inhale to around 60% of vital capacity, whereas at 70% it is only possible to inhale to around 35% of vital capacity. Adapted from Breathe Strong, Perform Better, Human Kinetics.
Inspiratory flow rate: To understand the advice below, it's necessary to have a quick "refresher" on the force-velocity relationship of muscle. Essentially this property dictates that the faster a muscle contracts, the lower the force it is able to generate and vice versa. An example of the force-velocity relationship at work is the difference in force one can exert on the pedals when cycling in a low gear, compared to a high gear.
This property can be exploited to optimise the training stimulus that the muscle receives. For example, assume that, because of the force-velocity relationship, as the rate of muscle contraction doubles, the force it can generate is halved, despite the same [maximal] effort being applied under both conditions. When muscles contract maximally at any speed, the number of muscle fibres that are recruited to the contraction is also maximised, despite the fact that faster contractions result in lower forces. Now consider the effect of doubling the rate of contraction slightly differently. When a muscle is contracting very slowly to move a load that requires, say, half its maximal force generating capacity, doubling the rate of contraction against the same load now requires ~100% of the muscle's force generating capacity (because its ability to generate force has been halved). This means that ~100% of the muscle fibres are recruited, for half the force. This can be turned to an advantage during IMT, because it means that it is possible to train close to 100% of a muscle's force generating capacity, no matter what load is being applied, provided that the load is moved as fast as possible (i.e., with maximal effort). Under any given loading condition, fast muscle contractions recruit more muscle fibres than slow contractions (Aagaard et al., 2000). Furthermore, recent evidence suggest that training improvements are maximised with higher velocities of muscle shortening (Padulo et al., 2012). Therefore, maximal effort ensures maximum velocity, and the recruitment of the greatest number of muscle fibres.
Muscle recruitment has an important impact on the response to training for two reasons. Firstly, fibres that are not recruited will not be trained. So, if the velocity of contraction is slow, a load requiring half of a muscle's force generating capacity will only require recruitment [and train] about half of its fibres; but if the same load is overcome as fast as possible, then close to 100% of fibres will be recruited and trained. Secondly, maximising recruitment is an important part of the neural adaption to training, which also contributes to optimising training outcomes. Training improves strength through two mechanisms, 1) stimulating muscle fibres to grow, 2) neural adaptations, which ensure that all available fibres within a muscles are recruited, and that all muscles that bring about a given movement are recruited.
In order to stimulate muscle hypertrophy, muscle fibres must be subjected to mechanical stress, which requires the application of at least moderate intensity loading. This is why high-velocity-low-load training does not improve strength, no matter how much effort is applied at low training loads. The practical implications of this for IMT are that strength and speed (power) can only be improved if the training load is at least moderate (50-60% of maximal strength), and the velocity of contraction (inhalation rate) is as fast as possible.
Accordingly, IMT should be conducted with maximum effort; i.e. each inhalation should be executed as fast as possible. This should take around 1-2 seconds and be accompanied by a loud rushing sound as air is sucked through the valve of the training device at high velocity. Encourage patients to make this sound as loud as possible, because this indicates high flow rates. Be aware that the heavier the relative load, the slower will be the maximal flow rate that can be generated (and the smaller the lung volume, see Figure 6.2). In contrast to the maximal nature of the inspiratory effort, exhalation should be passive, quiet, and require 3 to 4 seconds. Using an external breathing pacer that provides an auditory cue (link to App page) can be very helpful for supporting the process.
Because of the higher than normal breath volume and breathing frequency, some light-headedness may result from the hyperventilation-induced hypocapnia. This is harmless for the duration of a 30-breath session, and also seems to lessen in severity as training progresses (in patients with coronary artery disease, it is prudent to minimise hypocapnia by using slower breathing frequency and/or some rebreathing - see below). If dizziness is problematic, ask the patients to pause at the end of exhalation and wait for the urge to breathe in again. For maximal training overload, the training breaths should be completed as quickly as possible, but this has to be balanced against the effects of the hypocapnia. A method that can be used to overcome the loss of carbon dioxide is to place the training device inside a bag that has a slit down one side (a supermarket carrier bag is ideal). By rebreathing from the bag, the loss of carbon dioxide is largely abolished, and light-headedness is prevented. This allows patients to complete the breaths rapidly, maximising the training benefits.
Setting the training load
For people who are already feeling out of breath, the most challenging aspect of embarking on a programme of IMT is learning to tolerate the increased breathing effort that is inevitably associated with the training. This phase needs to be handled with particular sensitivity. A vital step in overcoming the anxiety that breathing through a resistance can provoke, is the realisation that the increased effort stops as soon as the training stops. So unlike the dyspnoea that one experiences during, say, climbing a flight of stairs, which can takes minutes to subside, the breathing effort of IMT ceases immediately the training device is removed. In addition, the sense of dyspnoea during IMT has a subtly different quality to that experienced during physical activity. The former is a sense of increased effort, whilst the latter also incorporates a sense of 'air hunger' that is akin to suffocation; hence the anxiety that it provokes. Practicing breathing through the training device in order to become familiar with the sensation, and its qualities, is a vital part of preparing a patient for IMT.
The next phase is to identify and set an appropriate training load, and the approach taken will depend upon whether there is access to equipment for assessing inspiratory muscle strength (maximal inspiratory pressure; MIP). If this is not available, then the "repetition maximum" (RM) principle is used to set the training load. Typically, a moderate load (50-60% of MIP) can be sustained for around 30 so breaths. Accordingly, the objective is to identify the 30RM and to train at the maximum load that can be sustained for only 30 breaths (this is explained further below). Patients, who are by definition unwell, may find even the lowest setting of the training device very challenging and be unable to complete 30 breaths without stopping. If this is the case, the load should remain at the lowest setting for the first week. Short breaks are allowable (and necessary for patients who need to cough), but should be minimised, otherwise the training stimulus will be diminished, or even lost completely.
Initially, the focus should be on inhaling deeply and forcefully, and exhaling slowly and gently. The objective in the first instance is to develop good breathing technique (see above) and to complete 30 breaths without the need to stop and rest. As soon as 30 breaths can be achieved without stopping, it's time to increase the training load by a quarter turn of the load tensioner (2-3 cmH2O) on a typical pressure threshold training device. Note that it may require a number of weeks for some severely compromised patients to achieve this (see below for Progressing training).
Some patients may find that they can complete more than 30 breaths easily at the lowest setting on day one. If this is the case, the load should be increased by one-quarter turn each day until a load is reached where 30 breaths is that maximum that can be achieved continuously. Once this load is reached, further increases in the training load should be made according to the guidance on Progressing training.
Where there is access to equipment for measuring MIP, the training load can be set using objective criteria. The training should commence at a load equivalent to 30-40% of MIP, provided that this is tolerable; this is the lowest intensity that has been shown to elicit improvements in function (Lotters et al., 2002). If this load is not tolerated, then commence training as described above until 30 breaths can be completed at the lowest setting. Most training devices do not have a calibrated scale printed on them, but many will provide a conversion chart that enables the level settings printed on the device to the cross-referenced to the corresponding load in cmH2O. Once the starting load of 30-40% can be tolerated, the load should be increased by one-quarter turn each day for the next 7-10 days, until up to 50-60% of baseline MIP is reached (see below for Progressing training).
Many patients experience life-changing results very quickly, and this can prompt such enthusiasm that they to want to train more than twice per day. This is definitely not advisable. Recovery is an important part of the training process, and the inspiratory muscles are already being subjected to a very challenging regimen of twice daily specific IMT. Do not be tempted to train more than twice daily, and ensure that the two sessions are separated by at least six hours.
Repetition Failure
Repetition failure is a slightly alien concept to people who have never engaged in any form of weight training. Essentially, it refers to the notion that at some point during repeated lifting of a weight, fatigue will make it impossible to lift the weight, resulting in "failure". Most weight training is undertaken to the point of failure, because this optimises the loading conditions that stimulate muscle adaptation (Toigo & Boutelier, 2006. For most muscles, the weakest point in the movement is at, or close to, the starting point. For example, when performing a bicep curl, the biceps are weakest at the onset of the exercise (when the elbow is extended), which means failure usually occurs at the start of the movement, with the result that the repetition cannot be started. In the case of the inspiratory muscles, the opposite is true; they are strongest at the start of the movement (at residual volume), becoming weaker as one inhales (see above). This means it may be possible to open the valve, but not possible to take a meaningful breath. So how should failure defined for IMT? A pragmatic approach is to tell the patients that once it's impossible to achieve a "satisfying breath", then failure has been reached and the session is complete. Some patients may require some encouragement in order to push themselves to this point, but it's the best way to achieve the results they are working towards. Notwithstanding this, it is not disastrous if patients only train until they have completed 30 breaths, provided that the training load is at least 60% of their current MIP, and the breathing technique described above is followed (maximising inspiratory flow and volume).
The influence of daily activities and exacerbations
Acute deteriorations in a patient's clinical condition, as well as other strenuous activities during the day, can affect the ease with which a training session can be completed. It's important that patients understand that there may be temporary setbacks. Some will be short-lived (over doing it physically on a particular day), but some will take some time to overcome (a exacerbation of COPD or asthma). In the case of the former, it's not usually necessary to reduce training loads, which should be avoided as much for the impact psychologically as physiologically. However, in the case of the latter, cessation of IMT is often required during an exacerbation, which means that training gains are lost, and the load must be reduced when training is recommenced. How soon should training recommence after an exacerbation? This is normally dictated by the patient's ability and enthusiasm for the training, but IMT should be recommenced as soon as possible, and certainly as soon as the patient is well enough to recommence the normal (for them) activities of daily living.
Use of training diaries
Keeping a training diary is an excellent way to keep track of the number of sessions completed, the increments in training load, the number of breaths completed, and how the session felt. This is an invaluable tool for both patient (e.g., enhancing motivation), and healthcare professional (e.g., monitoring compliance and progress). Some training devices provide a training diary in their user manuals (e.g., POWERbreathe® Medic).
Click here to download the Physiobreathe training diary template. As well as training load, etc., the template provides space for notes on how the training felt and other activities or health-related issues that may impact upon the training, as well as the patient's response to it. This facilitates cross-referencing of circumstances that may be helpful for the patient and healthcare professional in interpreting sudden up- or down-turns in training and/or symptoms.
Progressing Training:
Patients should be encouraged to train beyond 30 breaths if they feel able to, and can still achieve a "satisfying breath" (see Repetition Failure, above). In this way, they maximise progress. Once 30 continuous breaths can be completed, further increases in the training load should be made once per week, or as soon as 30 breaths can be exceeded. The increase in load should be sufficient to reduce the number of breaths that can be achieved before failure to between 25 and 30. On most training devices this will be about one quarter to one half turn on the spring tensioner. Bringing the number of breaths down to 25 is acceptable, because within a few days, the maximum number of breaths will be back up to 30. As a rough rule of thumb, the training load should be increased by at least one quarter turn each week for the first 8 to 12 weeks of training. Alternatively, small increases can be made as soon as the maximum number of breaths exceeds 33-35. If patients find that increasing the training load is too challenging, then they should be encouraged to focus on optimising their breathing technique during the training, i.e., maximising inspiratory flow rate and tidal volume. These measures can also increase the training stimulus, by increasing the power output achieved during the inhalation (maximising flow), and the work done (maximising volume).
If the patient is undertaking the training with the support of a clinician with access to equipment to measure inspiratory muscle strength (maximum inspiratory pressure; MIP), the load should be increased weekly to maintain the training load at 50-60% of the patients' new MIP.
The duration of the intensive, twice daily Foundation phase of training varies according to the circumstances in which the IMT is being undertaken, and the objectives. The first major consideration is whether the Foundation IMT is being undertaken as a standalone intervention, or as pat of the structured rehabilitation programme.Long term studies of standalone IMT in patients with COPD suggest that improvements in function occur most rapidly over the first 12 weeks, but continue for up to 12 months (Beckerman et al., 2005). These data suggest that duration of the Foundation phase of IMT should be at least 12 weeks.
Selection of the next phase of training depends upon a number of factors, including patient motivation, but there are essentially five options –
- Continue Foundation training for as long as the patient is motivated to do so. For some patients, changing a routine may create problems with respect to compliance. Alternatively, they may need more than 12 weeks before they feel ready to change.
- Enter the Maintenance training phase (see next section). Some patients may find the twice-daily Foundation routine onerous, in which case, moving to a Maintenance training regimen may retain their compliance.
- Enter the Functional training phase, which incorporates activities of daily living (link to Videos page). Motivated patients who have experienced good results during the Foundation phase may feel motivated to develop their training and to incorporate some functional elements to their daily regimen.
- Enter a rehabilitation programme, in which IMT is a component. Having undertaken a period of IMT, patients who were previously unable to benefit from exercise training may have recovered sufficient function to be able to enrol in a rehabilitation programme. In these patients, IMT can be continued in whatever form is most appropriate for the programme and the patient (Foundation, Maintenance or Functional).
If the benefits of IMT are to be retained, the intervention must be continued according to one of the options listed above. In circumstances where patients cease IMT completely at the end of the Foundation phase, it is possible to recover the benefits using periodic phases of foundation IMT. Ideally, IMT should resume before all of the benefits have regressed, as it is easier to recover post-training gains when starting from an elevated baseline. Data suggests complete regression of gains in MIP occurs over a period of around 12 months (Weiner et al., 2004). However, it appears that around half of the strength gained is retained for up to 12 weeks. This magnitude of improvement is probably at the threshold of what is required in order to elicit enhancement of exercise tolerance and reduction in dyspnoea. Accordingly, 12 weeks probably represents the maximum period that should be permitted before recommencing IMT. It is also possible, though not proven experimentally, that the duration of the IMT during these periodic bouts of training can be shorter. Thus, a design for a periodic training regimen might be 12 weeks of Foundation IMT, followed by repeated cycles of 12 weeks of detraining and 6 weeks of Foundation IMT.
Whether Foundation IMT is being used as a standalone intervention, or as part of a rehabilitation programme, its duration should ideally be 12 weeks, since this represents the period during which the largest improvements in function are gained. However, this does not mean that briefer periods of Foundation training are worthless, far from it. The duration of many pulmonary rehabilitation programmes, is typically 6-12 weeks, thus, there may be logistical issues relating to the duration of the Foundation phase and its relationship to the rehabilitation programme. In an ideal scenario where the Foundation phase has a 12-week duration, this should be dovetailed with the rehabilitation programme.
Maintenance training:
Once the Foundation phase of training has been completed, some patients are perfectly satisfied with the results that they have achieved, and are content to enter a phase of maintenance training. Research has shown that training frequency can be reduced by as much as two thirds without any loss of functional benefits (Weiner et al., 2004). In other words, training can switch from twice daily, to training once, every other day. There is, of course, no reason at all that someone cannot switch directly from maintenance training into Functional training if they so wish.
Foundation IMT Essentials
- Use a training load of 50-60% of MIP, or set it to the 30-repetition maximum (30RM) using a process of trial and error.
- Use stretching and warm-up to prepare for IMT.
- Inhale against the load with maximum effort (as fast as possible).
- Breathe in AND out as far as possible during each breath.
- Train twice per day—morning and evening.
- Remember that repetition failure for the inspiratory muscles is an "inability to achieve a satisfying breath."
- Increase the training load at least once per week.
- Progress the training by, 1) maintaining it at 50-60% of the new MIP, or 2) keeping the load at the new 30RM to account for improvement.
- Train to "failure" in a window between 25 and 35 breaths per session.
- Keep in mind that time of day, other activities, and health status may affect IMT because of residual fatigue. Accordingly, evening IMT sessions may be more challenging than morning sessions—but don't reduce the training load.
- If you suspect that there is any residual fatigue of the inspiratory muscles, take a day off from IMT.
- Keep an IMT diary.
If you found this section useful, then find out more in the comprehensive guide to respiratory muscle training – 'Respiratory muscle training: theory and practice'. Follow this link to purchase.
FREE Trial >
![]() Thanks to a unique partnership with PhysioTec, purchasers of
"Respiratory Muscle Training: theory and practice" can build bespoke patient protocols,
using Physiotecs online library of over 150 functional respiratory training exercises.
Thanks to a unique partnership with PhysioTec, purchasers of
"Respiratory Muscle Training: theory and practice" can build bespoke patient protocols,
using Physiotecs online library of over 150 functional respiratory training exercises.
More >
The Book >
 Respiratory Muscle Training: theory & practice is the world's
first book to provide an "everything-you- need-to-know" guide to respiratory muscle training.
Respiratory Muscle Training: theory & practice is the world's
first book to provide an "everything-you- need-to-know" guide to respiratory muscle training.
More >
The Author >
 Professor Alison McConnell is the world's leading expert on respiratory
muscle training and the creator of the market-leading POWERbreathe® inspiratory muscle trainers.
Professor Alison McConnell is the world's leading expert on respiratory
muscle training and the creator of the market-leading POWERbreathe® inspiratory muscle trainers.
More >
Videos >
 Access selected videos of functional
respiratory training exercises from "Respiratory Muscle Training: theory and practice".
Access selected videos of functional
respiratory training exercises from "Respiratory Muscle Training: theory and practice".
More >